

Most discussions surrounding breast surgery focus on aesthetics, yet the longevity of your result is dictated by a silent force: breast augmentation biomechanics. Gravity does not negotiate with your skin; it works against the weight of the implant every second. If the surgical architecture ignores the load-bearing capacity of your pectoralis major fascia, even the most beautiful initial result can lead to “bottoming out” or glandular ptosis within years.
Understanding the internal physics of your procedure is the only way to move beyond temporary “looks” toward a lifetime of structural integrity. This masterclass shifts the focus from cup sizes to the 2026 taxonomy of surgical planes, empowering you to choose a path that preserves your anatomy while achieving your aesthetic goals. By mastering these principles, you ensure your surgical investment withstands the biological shifts of aging and tissue elasticity.

The Pectoralis Major Fascia: Your Body’s Natural Internal Suspension
In traditional surgery, the muscle was often viewed merely as a cover. Today, we recognize the pectoralis major fascia as the primary load-bearing element in breast augmentation biomechanics. This thin but resilient layer of connective tissue acts as a biological “internal bra.” When an implant is placed with intentional preservation of this fascia, the risk of lateral displacement is drastically reduced.
The interaction between the implant and the submuscular environment creates a dynamic tension. This tension must be balanced; too much pressure from the muscle can cause “animation deformity,” while too little support leads to the implant migrating south. Successful outcomes rely on the surgeon’s ability to navigate the ‘dual-plane transition,’ ensuring the implant is supported by muscle superiorly while allowing the gland to drape naturally inferiorly. You can explore our philosophy on individualized care at About Us.

2026 Taxonomy of Surgical Planes: Beyond Subglandular and Submuscular
The choice of where to house the implant is the most critical architectural decision in your surgery. We no longer speak in binary terms of “above or below” the muscle. The 2026 standard utilizes a nuanced spectrum tailored to your glandular tissue density and skin quality.
| Surgical Plane | Biomechanical Advantage | Ideal Candidate |
|---|---|---|
| Subglandular Pocket | Zero animation deformity; faster recovery. | Thick glandular tissue; minimal ptosis. |
| Dual-Plane Type I | Upper pole coverage with natural lower pole expansion. | Athletic builds with tight skin. |
| Dual-Plane Type II/III | Corrects mild glandular ptosis by releasing muscle attachments. | Post-pregnancy tissue laxity. |
| Subfascial | Enhanced edge masking without muscle disruption. | Thin patients needing extra coverage. |
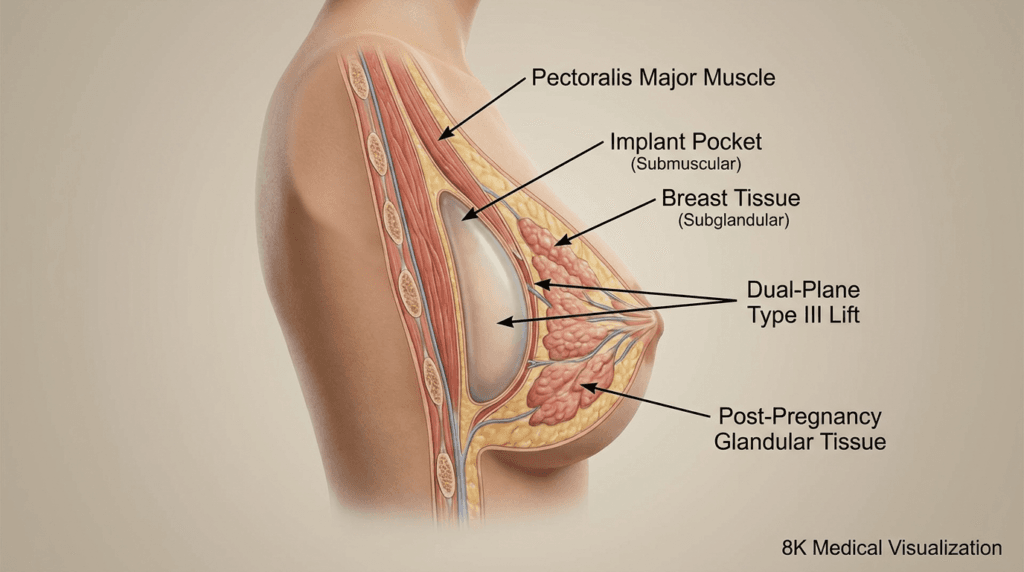
The Dual-Plane Technique (Type I-III)
The dual-plane approach is the gold standard for harmonizing breast augmentation biomechanics. By varying the degree of muscle release (Types I, II, or III), the surgeon can precisely control how the implant interacts with the breast gland. In Type III releases, used often in cases of “pseudo-ptosis,” the muscle is detached more extensively to allow the implant to sit directly behind the nipple-areola complex, effectively lifting the tissue from within without the need for large external incisions.
Inframammary Fold (IMF) Stability
The “foundation” of your breast is the inframammary fold. Biomechanically, if the IMF is compromised during surgery, the implant will slide down the chest wall—a complication known as “bottoming out.” Modern techniques prioritize “no-touch” IMF preservation, using the natural ligamentous attachments to lock the implant in its intended position. Maintaining this structural “shelf” is vital for patients traveling for international health tourism, where long-term stability is the highest priority.
Implant Architecture: Volume vs. Projection Physics
Not all volumes are created equal. The biomechanical impact of a 300cc “High Profile” implant is vastly different from a 300cc “Low Profile” implant. High projection implants exert more forward pressure on the skin envelope (thinning it over time), whereas wider base implants distribute weight more evenly across the chest wall. Selecting the right architecture requires a practitioner-level observation of your glandular tissue density and chest wall width.
- Glandular Ptosis Grading: We assess the degree of sag to determine if the biomechanics of an implant alone can “lift” the breast or if a mastopexy is required.
- Cohesive Gel Integrity: Modern 2026 implants use “form-stable” gels that maintain their shape even under the pressure of the pectoralis major muscle, preventing the “collapsed” look of older generations.

Your Roadmap to Structural Success
Moving from theory to practice requires a calculated approach to your surgical journey. Follow these steps to ensure your breast augmentation biomechanics are sound:
- Assess Tissue Pinch Test: Measure the thickness of your upper breast tissue. If it is less than 2cm, submuscular or subfascial placement is usually necessary to prevent visible implant edges.
- Define Your Activity Level: High-impact athletes may benefit from specific subglandular or subfascial planes to avoid muscle-related implant movement during exercise.
- Evaluate IMF Position: Determine if your natural fold is symmetrical. A surgeon must biomechanically “reset” or “reinforce” these folds during the procedure.
- Consult with an Expert: Ensure your surgeon understands the nuances of dual-plane transitions and fascial preservation.
Precision in breast augmentation biomechanics is the difference between a result that lasts five years and one that lasts twenty. If you are ready to prioritize the structural health of your body alongside your aesthetic transformation, we invite you to schedule your consultation today at our Antalya clinic.
Frequently Asked Questions
How do biomechanics affect the feel of the breast?
The biomechanics of implant placement dictate tissue tension. Submuscular placement often feels firmer initially because of muscle pressure, while subglandular or dual-plane techniques tend to mimic the natural softness of breast tissue more closely as the muscle relaxes over time.
Why is the pectoralis major fascia so important?
The fascia acts as a structural anchor. By keeping this layer intact, the surgeon provides a stable environment for the implant, preventing it from shifting toward the armpit or sinking too low, which preserves the natural silhouette for much longer.
What happens if the biomechanical load is too heavy?
If an implant is too heavy for the skin’s elastic threshold, the tissue will stretch and thin. This leads to visible rippling and glandular ptosis. Selecting an implant that matches your body’s load-bearing capacity is vital for long-term health.
Can biomechanics fix asymmetrical breasts?
Yes, by using different surgical planes or implant architectures for each breast, a surgeon can balance the biomechanical forces. This ensures that both breasts settle and age at the same rate, maintaining symmetry over the years.





